Saudi hospitals have made real progress on digital transformation—but the next efficiency gains will come from intelligence, not more digitisation.
In practical terms, the Kingdom now has a growing digital care layer (e.g., SEHA Virtual Hospital supports around 224 hospitals and is designed for large-scale virtual service delivery) and mass patient-facing uptake (the Sehhaty app reports 31M+ registered users).
Digitization mainly helps make data more visible and easier to document. But it does not automatically stop revenue leakag, fix complicated scheduling, or reduce mistakes in billing and insurance claims that hurt profits.
This gap is becoming more important as the number of transactions between healthcare payers and providers increases, along with stricter compliance rules around data they need to follow.
That’s why Saudi Arabia is pushing for standardization efforts like NPHIES, where reports say that 75% of private healthcare providers are connected, with a goal to reach 91% connectivity through digital systems.
This is where hospital AI centres matter: they are not PR labs, but operating engines that turn digital data into measurable financial outcomes—higher capacity utilisation, a reduction in the number of insurance claims that are rejected by insurance companies, tighter billing accuracy, and lower operational risk.
Saudi Arabia already has a flagship example of what advanced digital and AI governance in healthcare can look like. King Faisal Specialist Hospital and Research Centre (KFSHRC) has spent several years building an internal digital and AI ecosystem, anchored by a dedicated innovation and intelligence function. Its model shows that AI can be embedded at scale rather than treated as a series of disconnected pilots.
KFSHRC remains the exception, not the norm. A recent independent study at one of the publications of Springer Nature found that only 2 out of 34 major hospitals in Saudi Arabia have established formal AI centres—an adoption rate of just 5.88%.
This gap is not explained by a lack of strategic intent, but by structural constraints: cost, regulatory complexity, and limited internal capability.
Crucially, widespread digitisation alone has not closed this gap. Electronic medical records, billing systems, and scheduling platforms have improved documentation and compliance, but they remain largely reactive.
They record what has already happened, rather than predicting no-shows, identifying systematic billing leakage, or flagging denial risk before it materialises. As transaction volumes grow and reimbursement rules become more complex, these limitations translate directly into margin pressure and cash-flow volatility.
The contrast is therefore clear. KFSHRC demonstrates what is institutionally possible, while the low national adoption rate highlights why a purely digitisation-led approach is insufficient to deliver system-wide efficiency gains.
ℹ︎
Eyes on the Past, Missing the Future
● Limited Predictive Capabilities
Digital systems primarily record past events. ●Reactive Operational Focus Digitalisation does not facilitate real-time decision-making. ●Increased Margin Pressure
Digitalisation does not enable early corrective actions that preserve margins. ● Cash-Flow Volatility Due to the lack of predictive insight into billing denials or emerging compliance issues.
The Economic Case for Hospital AI Centers
The economic case for a hospital AI centre is simple: it targets the largest silent drags on cashflow and margins—capacity waste, revenue leakage, and avoidable operational risk—using the data hospitals already collect.
AI can protect capacity utilisation, especially in outpatient care. Digitised booking systems can log non-attendance, but they cannot reliably predict it.
NHS England’s rollout of an AI tool followed a pilot that cut Did Not Attends (DNA) by almost a third in six months, releasing real capacity without adding staff or clinics.
(Other reporting puts the scale of the problem at millions of missed appointments annually, underlining the size of the efficiency prize.)
AI centers help remove delays and blockages in the hospital’s flow of patients and work, which can limit how many patients are treated and how much money the hospital makes.
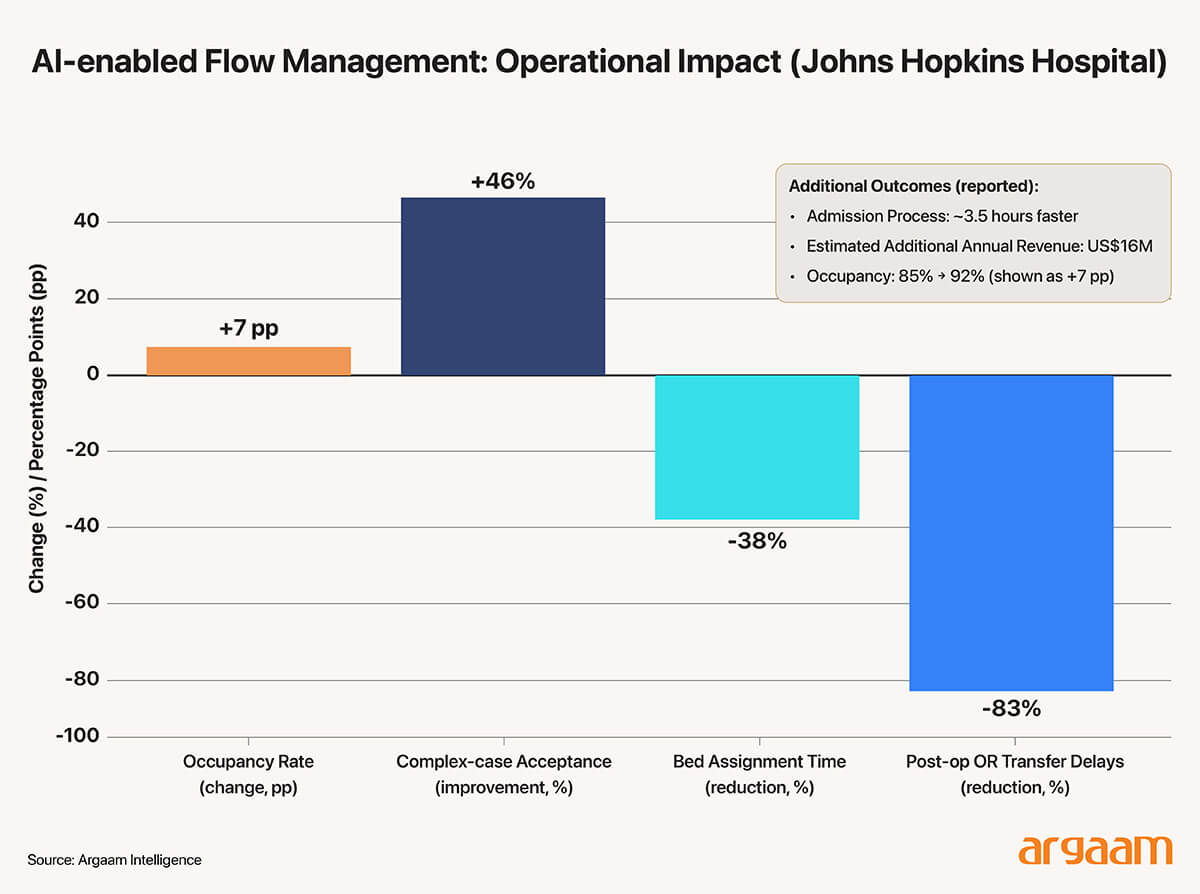
At Johns Hopkins Hospital in the US, they set up a special data-based command center that focused on the whole system. This significantly improved how well the entire hospital system worked, not just separate departments.
Reported outcomes included an increase in average occupancy rates from 85% to 92%, achieved alongside a reduction in patient delays, and a 46% improvement in the hospital’s ability to accept patients with complex medical conditions.
Bed assignment times were cut by 38%, accelerating the admission process by approximately 3.5 hours once a decision to admit had been made. In perioperative care, operating-room transfer delays following procedures fell by 83%.
Collectively, these improvements translated into an estimated $16 million in additional annual revenue, illustrating how AI-enabled flow management converts operational efficiency into tangible financial returns.
dominated by large, vertically integrated producers with modern farms, processing capacity, and national cold-chain distribution.
Note “Low upside” refers to the capped returns of isolated digital or AI initiatives, while “stage-gated ROI” describes a phased deployment model where each expansion is justified by proven financial outcomes.
AI can strengthen the hospital's revenue process. It can be used in useful ways like automatically helping with coding, checking claims for mistakes before they are submitted, and predicting which claims might be denied so they can be fixed early. This makes billing and handling denials go from being a last-minute fix to a proactive part of the process.
In this framing, an AI centre is not a showcase lab. It is a margin-protection function that converts operational noise into measurable financial outcomes.
showing that the country has moved well beyond relying on small farms or individual farmers. Overall, Saudi Arabia’s food security data indicates that the country has a plentiful and sufficient supply of dairy products.
Why Hospital AI Stalls, Not Fails
AI in hospitals does not fail because the algorithms are immature. It stalls because adoption is a capital allocation + incentives + risk-pricing problem.
Hospitals can only capture AI’s “system-level” benefits when someone is willing to fund uncertain upfront build-out, tolerate early-stage iteration, and pay for the governance needed to deploy models safely in real workflows.
This is where public healthcare systems encounter fundamental challenges. Large AI projects require significant upfront investments, such as integrating data, redesigning workflows, hiring talent, and ensuring cybersecurity.
However, in many government-run systems, success often isn’t recognized or rewarded adequately, while failures are highly visible and subject to intense scrutiny from audits. This creates a bias among decision-makers to favor safer, small improvements instead of riskier, bigger investments that could have greater payoff.
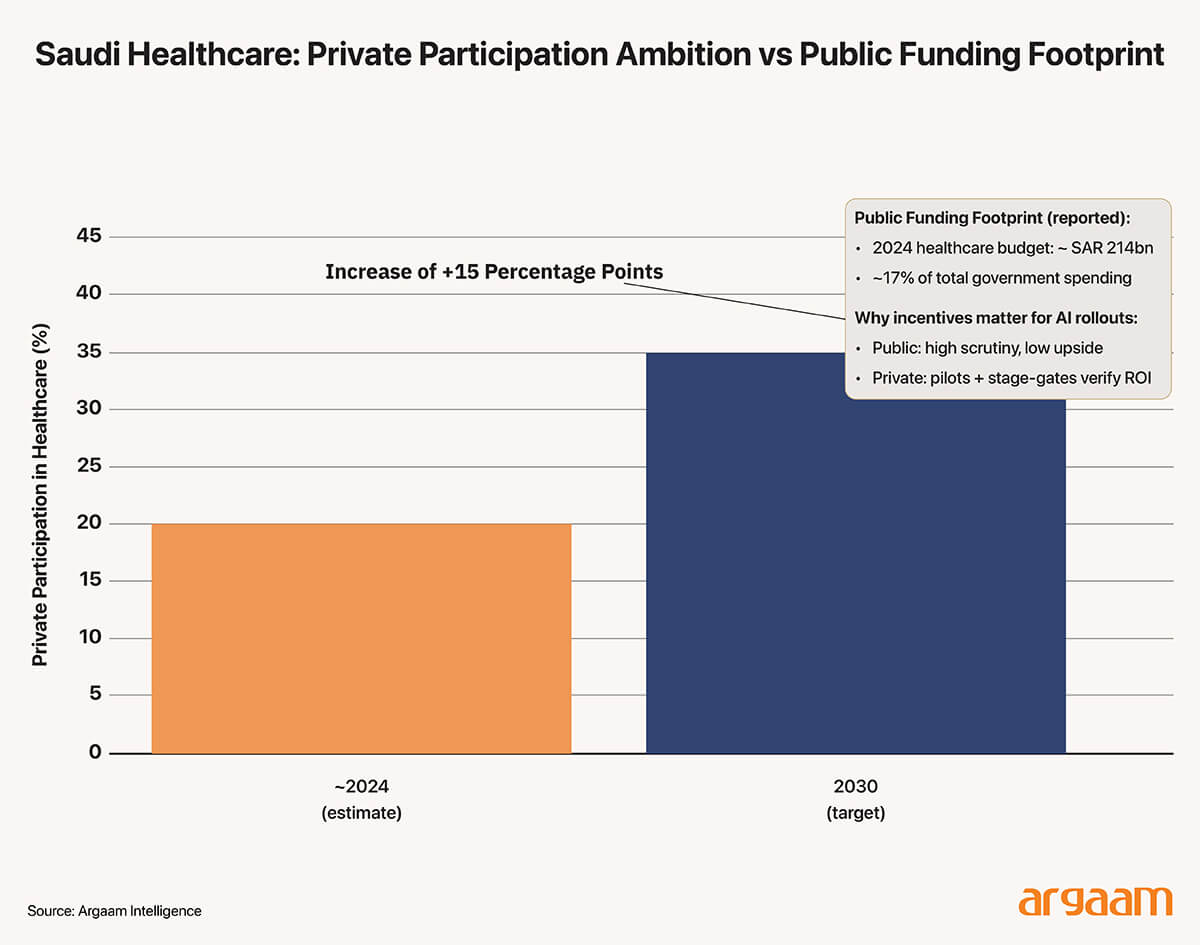
In Saudi Arabia, that caution sits alongside a very large public funding footprint: industry briefings, for example, have cited a 2024 healthcare budget of SAR 214bn (around 17% of total government spending), underscoring both the scale of the system and the pressure for disciplined spend.
By contrast, when incentives are tied directly to margins and cashflow stability, the adoption logic changes. Modular rollouts keep costs controllable, small pilots make ROI verifiable, and repeatable playbooks support scalable valuation.
That is why “capital can solve the cost problem” not simply by spending more, but by enabling managed experimentation and stage-gated scaling—a pattern aligned with the Kingdom’s stated aim to raise private participation in healthcare from 20% to at least 35% by 2030.
ℹ︎
Capital roadblocks
● Funding Hesitation
Public hospitals are reluctant to allocate large capital upfront ● Incentive Misalignment
Decision makers favor smaller, safer improvements ● Early-stage Uncertainty
Initial deployment often face setbacks ● Risk-Pricing Gaps
Current funding methods don't properly account for the future advantages of AI projects
Pilot Programs that Deliver Real Economic Value
A consistent lesson from early adopters is that AI success in healthcare is not a big-bang rollout but a staged, evidence-driven progression.
The most resilient implementations start with small, tightly scoped use cases that deliver measurable ROI and then expand outward once value is validated.
This calibrated approach avoids the common trap of deploying AI without a foundation of trusted data or clear operational goals, which is why many broad initiatives stall even when individual technologies are powerful.
The first phase is targeted pilots focused on pain points with clear economic impact—such as scheduling optimisation, denial prediction, or documentation automation.
These are the kinds of point solutions that can be easily scoped, integrated with existing systems, and evaluated against concrete KPIs (e.g., reduced processing time or fewer denials).
Notably, industry research shows the next frontier of healthcare AI is one where early tactical applications become the building blocks for a modular connected architecture, rather than isolated tools that never scale.
Once a pilot delivers ROI—either by reducing cost, increasing throughput, or stabilising cashflow—the organisation can expand gradually by integrating additional modules or scaling to more departments or facilities. This path mitigates risk and generates a track record of measurable outcomes that justify further investment.
A key enabler in this pathway is reliable digital infrastructure. Without trusted, governed data and interoperable systems, AI pilots struggle to scale. Thought leaders in healthcare analytics emphasise that transforming fragmented data into contextual, explainable insights is a prerequisite for scalable AI value creation; a structured roadmap from fragmented data to trusted intelligence significantly raises the likelihood that initial pilots will succeed and expand.
Our earlier discussion in this analysis highlighted that AI’s biggest gains come when models and workflows operate at systemic scale, not merely as isolated point solutions.
However, it’s important to underscore the critical distinction between pilots and true end states. In complex healthcare environments, pilots are not the destination; they are economic proof mechanisms—designed to validate ROI, mitigate risk, and build the governance muscle necessary for broader adoption.
A single hospital’s attempt to build its own AI centre illustrates why pilots alone rarely deliver system-level effects without further design. The challenges can be summed up in the coming table:
Challenge
Description
Time Frame
High upfront costs
Significant capital for data systems
Initial phase
Limited data
Small datasets limit model accuracy and generalization
Short to medium term
Talent constraints
Scarcity and high cost of AI specialists
Ongoing
Concluding thought
These challenges suggest using shared AI platforms. In these models, a single AI tool—like software, data analysis, or prediction systems—is paid for once and then used by many hospitals.
Sharing the platform helps distribute the costs among multiple users and enables the AI to learn from a larger variety of data from different hospitals. Importantly, this approach avoids the need to gather all the raw data in one place.
This technique enables many hospitals to collaborate in training a common AI model, but each keeps its sensitive patient information safely stored at its own location.
The most feasible trajectory combines private-led AI platform development with public governance adoption. Private operators can invest and iterate to prove economic value, while public partners provide the governance frameworks necessary to integrate these capabilities at scale.
More this Weekend
M&As in US, Europe and GCC: Analysing Transaction Mindsets that Shape Deal Structures
In today’s M&A environment, deal structuring has become a central lever for both value creation and risk management. In the US and Europe, transactions particularly in the mid-market remain predominantly sponsor-driven, highly leveraged and control focused.
Understanding Saudi Arabia’s 11.2% Household Savings Rate: A Positive Sign of Prudence But Underlying Financial Complexities Remain
Saudi Arabia's 2023 Household Income and Expenditure Survey, which’s the latest available dataset and is our baseline in our argument, reveals average monthly household disposable income of SAR 18,056 and consumption of SAR 16,028, implying an 11.2% savings rate—dramatically higher than 2018's 1.6% (—approximately 749% increase in absolute savings).